
History
DNP ÆRESMEDLEM 2015 – Ole Didrik Lærum.
Den Norske Patologforening. 50 års jubileum. 1923-1973.
Den Norske Patologforening. 75 års Jubileum. 1923-1998.
Rettsmedisinsk Institutt 50 år. Professor Jon Lundevall.
Noen kjente norske patologer
Norske patologer i internasjonalt historieverk. Den norske patologforening.
DNP, Den Norske Patologforening. Norwegian Society of Pathology
Årsrapport 2020: https://www.legeforeningen.no/globalassets/foreningsledd/fagmedisinske-foreninger/den-norske-patologforening/arsrapport-dnp-2020_.pdf
Utland
List of pathologists https://en.wikipedia.org/wiki/List_of_pathologists
100 Jahre Hautklinik | Heidelberg
Albert Bernard Ackerman 1936 2008. Dermatopathology
Hippokrates’ ed
Fra: Anfinn Stigen, «Tenkningens historie» (Gyldendal 1983, ISBN 82-05-14663-2):
Jeg sverger ved Apollon, ved Asklepios, ved Helsen, ved Panakeia og ved alle guder og gudinner, idet jeg gjør dem til mine vitner over at jeg vil gjennomføre, i samsvar med min dyktighet og dømmekraft, denne ed og denne lære.
Jeg vil sette min læremester like høyt som mine egne foreldre, gjøre ham deltagende i mitt levebrød, når han trenger penger dele mine med ham, betrakte hans familie som mine egne brødre og lære dem denne kunst – hvis de ønsker å lære den – uten belønning, å gi lærdom, muntlig anvisning og alle slags råd til mine egne barn, til min læremesters barn og til elever som har avlagt legeeden, men ikke til noen andre.
Jeg vil bruke behandling for å hjelpe syke i samsvar med mine evner og vurderinger, men aldri med henblikk på å skade eller gjøre vondt. Jeg vil hverken gi giftig medisin til noen som ber om det eller oppfordre til dette. Likeså vil jeg ikke gi en kvinne pessar for å forhindre svangerskap. Jeg vil holde både mitt liv og min kunst ren og hellig.
Jeg vil ikke bruke kniven, ikke engang på dem som lider uutholdelig, men jeg vil gi plass til dem som er fagfolk på dette området.
Samme hvilket hus jeg går inn i, vil jeg gå dit for å hjelpe de syke, og jeg vil avstå fra all forsettelig urett og skade, spesielt fra å misbruke kroppen til en mann eller kvinne, trell eller fri. Hva jeg enn får se eller høre i mitt samkvem med mennesker, hvis det er noe som ikke skal gjøres kjent for andre, vil jeg aldri avsløre det, idet jeg holder slike ting som hellige hemmeligheter.
Hvis jeg gjennomfører denne ed og ikke bryter den, la meg for alltid nyte anseelse blant menneskene for mitt liv og for min kunst. Men hvis jeg bryter eden og forsverger meg, la det motsatte skje meg.
OATH AND LAW OF HIPPOCRATES
From “Harvard Classics Volume 38” Copyright 1910 by P.F. Collier and Son.
THE OATH OF HIPPOCRATES
I SWEAR by Apollo the physician and AEsculapius, and Health, and All-heal, and all the gods and goddesses, that, according to my ability and judgment, I will keep this Oath and this stipulation — to reckon him who taught me this Art equally dear to me as my parents, to share my substance with him, and relieve his necessities if required; to look upon his offspring in the same footing as my own brothers, and to teach them this art, if they shall wish to learn it, without fee or stipulation; and that by precept, lecture, and every other mode of instruction, I will impart a knowledge of the Art to my own sons, and those of my teachers, and to disciples bound by a stipulation and oath according to the law of medicine, but to none others. I will follow that system of regimen which, according to my ability and judgement, I consider for the benefit of my patients, and abstain from whatever is deleterious and mischievous. I will give no deadly medicine to any one if asked, nor suggest any such counsel; and in like manner I will not give to a woman a pessary to produce abortion. With purity and with holiness I will pass my life and practice my Art. I will not cut persons labouring under the stone, but will leave this to be done by men who are practitioners of this work. Into whatever houses I enter, I will go into them for the benefit of the sick, and will abstain from every voluntary act of mischief and corruption; and, further, from the seduction of females or males, of freemen and slaves. Whatever, in connection with my professional service, or not in connection with it, I see or hear, in the life of men, which ought not to be spoken of abroad, I will not divulge, as reckoning that all such should be kept secret. While I continue to keep this Oath unviolated, may it be granted to me to enjoy life and the practice of the art, respected by all men, in all times. But should I trespass and violate this Oath, may the reverse be my lot.
THE LAW OF HIPPOCRATES
1. Medicine is of all the arts the most noble; but, owing to the ignorance of those who practice it, and of those who, inconsiderately, form a judgment of them, it is at present far behind all the other arts. Their mistake appears to me to arise principally from this, that in the cities there is no punishment connected with the practice of medicine (and with it alone) except disgrace, and that does not hurt those who are familiar with it. Such persons are the figures which are introduced in tragedies, for as they have the shape, and dress, and personal appearance of an actor, but are not actors, so also physicians are many in title but very few in reality.
2. Whoever is to acquire a competent knowledge of medicine, ought to be possessed of the following advantages: a natural disposition; instruction; a favorable position for the study; early tuition; love of labour; leisure. First of all, a natural talent is required; for, when Nature leads the way to what is most excellent, instruction in the art takes place, which the student must try to appropriate to himself by reflection, becoming an early pupil in a place well adapted for instruction. He must also bring to the task a love of labour and perseverance, so that the instruction taking root may bring forth proper and abundant fruits.
3. Instruction in medicine is like the culture of the productions of the earth. For our natural disposition, is, as it were, the soil; the tenets of our teacher are, as it were, the seed; instruction in youth is like the planting of the seed in the ground at the proper season; the place where the instruction is communicated is like the food imparted to vegetables by the atmosphere; diligent study is like the cultivation of the fields; and it is time which imparts strength to all things and brings them to maturity.
4. Having brought all these requisites to the study of medicine, and having acquired a true knowledge of it, we shall thus, in travelling through the cities, be esteemed physicians not only in name but in reality. But inexperience is a bad treasure, and a bad fund to those who possess it, whether in opinion or reality, being devoid of self-reliance and contentedness, and the nurse both of timidity and audacity. For timidity betrays a want of powers, and audacity a lack of skill. They are, indeed, two things, knowledge and opinion, of which the one makes its possessor really to know, the other to be ignorant.
5. Those things which are sacred, are to be imparted only to sacred persons; and it is not lawful to impart them to the profane until they have been initiated into the mysteries of the science.
(HIPPOCRATES,
the celebrated Greek physician, was a contemporary of the historian Herodotus. He was born in the island of Cos between 470 and 460 B.C., and belonged to the family that claimed descent from the mythical AEsculapius, son of Apollo. There was already a long medical tradition in Greece before his day, and this he is supposed to have inherited chiefly through his predecessor Herodicus; and he enlarged his education by extensive travel. He is said, though the evidence is unsatisfactory, to have taken part in the efforts to check the great plague which devastated Athens at the beginning of the Peloponnesian war. He died at Larissa between 380 and 360 B.C.
The works attributed to Hippocrates are the earliest extant Greek medical writings, but very many of them are certainly not his. Some five or six, however, are generally granted to be genuine, and among these is the famous “Oath.” This interesting document shows that in his time physicians were already organized into a corporation or guild, with regulations for the training of disciples, and with an esprit de corps and a professional ideal which, with slight exceptions, can hardly yet be regarded as out of date.
One saying occurring in the words of Hippocrates has achieved universal currency, though few who quote it to-day are aware that it originally referred to the art of the physician. It is the first of his “Aphorisms”: “Life is short, and the Art long; the occasion fleeting; experience fallacious, and judgment difficult. The physician must not only be prepared to do what is right himself, but also to make the patient, the attendants, and externals cooperate.”).
Rudolf Virchow (“uttales wircho”!)
* 1821 + 1902
Tysk patolog
Grunnlegger av cellularpatologi !
Grunnleggende undersøkelser angående patologisk anatomi
Svulstforskning
Forkjemper for hygiene
Politiker


Rudolf Virchow, Cellularpathologie. Berlin 1858.
Internetausgabe der Vorrede und der ersten Vorlesung
von Thomas Gloning und Christian Heuer. Marburg 2000.
[1] = Seitenzahl, [1Anm] = Seitenzahl von Abbildungskommentaren, die im Original jeweils am Fuß der betreffenden Seite stehen;
die römischen Seitenzahlen beziehen sich auf den Nachdruck 1966.
CELLULARPATHOLOGIE
in ihrer Begründung auf
physiologische und pathologische Gewebelehre.
———————
Zwanzig Vorlesungen,
gehalten
während der Monate Februar, März und April 1858 im pathologischen
Institute zu Berlin
von
Rudolf Virchow,
o.ö. Prof. der pathologischen Anatomie, der allgemeinen Pathologie u. Therapie an der
Universität, Direktor des patholog. Instituts u. dirigirendem Arzte a. d. Charité.Mit 144 Holzschnitten.
BERLIN, 1858.
Verlag von August Hirschwald.
69 Unter den Linden (Ecke der Schadowstr.).
[XI] Vorrede.
Die Vorlesungen, welche ich hiermit dem weiteren
ärztlichen Publicum vorlege, wurden im Anfange
dieses Jahres vor einem grösseren Kreise von Collegen,
zumeist praktischen Aerzten Berlin’s, in dem
neuen pathologischen Institute der Universität gehalten.
Sie verfolgten hauptsächlich den Zweck, im
Anschlusse an eine möglichst ausgedehnte Reihe von
mikroskopischen Demonstrationen eine zusammenhängende
Erläuterung derjenigen Erfahrungen zu gehen,
auf welchen gegenwärtig nach meiner Auffassung die
biologische Doctrin zu begründen und aus welchen
auch die pathologische Theorie zu gestalten ist. Sie
sollten insbesondere in einer mehr geordneten Weise,
als dies bisher geschehen war, eine Anschauung von
der cellularen Natur aller Lebenserscheinungen, der
physiologischen und pathologischen, der thierischen
und pflanzlichen zu liefern versuchen, um gegenüber
den einseitigen humoralen und neuristischen (solidaren)
Neigungen, welche sich aus den Mythen des Alterthums
bis in unsere Zeit fortgeflanzt [!] haben, die Einheit
des Lebens in allem Organischen wieder dem Bewusstsein
näher zu bringen, und zugleich den ebenso
einseitigen Deutungen einer grob-mechanischen und
chemischen Richtung die feinere Mechanik und Chemie
der Zelle entgegen zu halten.
[XII] Bei den grossen Fortschritten des Einzelwissens
ist es der Mehrzahl der praktischen Aerzte immer
schwieriger geworden, sich dasjenige Maass der eigenen
Anschauung zu gewinnen, welches allein eine gewisse
Sicherheit des Urtheils verbürgt. Täglich entschwindet
die Möglichkeit nicht bloss einer Prüfung,
sondern selbst eines Verständnisses der neueren Schriften
denjenigen mehr und mehr, welche in den oft so
mühseligen und erschöpfenden Wegen der Praxis ihre
beste Kraft verbrauchen müssen. Denn selbst die
Sprache der Medicin nimmt allmählig ein anderes
Aussehen an: bekannte Vorgänge, welche das herrschende
System seinem Gedankenkreise an einem bestimmten
Orte eingereiht hatte, wechseln mit der Auflösung
des Systems die Stellung und die Bezeichnung.
Indem eine gewisse Thätigkeit von dem Nerven, dem
Blute oder dem Gefässe auf das Gewebe verlegt,
ein passiver Vorgang als ein activer, ein Exsudat als
eine Wucherung erkannt wird, ist auch die Sprache
genöthigt, andere Ausdrücke für diese Thätigkeiten,
Vorgänge und Erzeugnisse zu wählen, und je vollkommener
die Kenntniss des feineren Geschehens der
Lebensvorgänge wird, um so mehr müssen sich auch
die neueren Bezeichnungen an diese feineren Grundlagen
der Erkenntniss anschliessen.
Nicht leicht kann Jemand mit mehr Schonung
des Ueberlieferten die nothwendige Reform der Anschauungen
durchzuführen versuchen, als ich es mir
zur Aufgabe gestellt habe. Allein die eigene Erfahrung
hat mich gelehrt, dass es hier eine gewisse
Grenze gibt. Zu grosse Schonung ist ein wirklicher
Fehler, denn sie begünstigt die Verwirrung: ein
zweckmässig gewählter Ausdruck macht dem allgemeinen
[XIII] Verständnisse etwas sofort zugänglich, was ohne
ihn jahrelange Bemühungen höchstens für Einzelne
aufzuklären vermochten. Ich erinnere an die parenchymatöse
Entzündung, an Thrombose und Embolie,
an Leukämie und Ichorrhämie, an osteoides und
Schleimgewebe, an käsige und amyloide Metamorphose,
an die Substitution der Gewebe. Neue Namen sind
nicht zu vermeiden, wo es sich um thatsächliche
Bereicherungen des erfahrungsmässigen Wissens handelt.
Auf der anderen Seite hat man es mir schon öfters
zum Vorwurfe gemacht, dass ich die moderne Anschauung
auf veraltete Standpunkte zurückzuschrauben
bemüht sei. Hier kann ich wohl mit gutem Gewissen
sagen, dass ich eben so wenig die Tendenz habe, den
Galen oder den Paracelsus zu rehabilitiren, als ich
mich davor scheue, das, was in ihren Anschauungen
und Erfahrungen wahr ist, offen anzuerkennen. In der
That finde ich nicht bloss, dass im Alterthum und im
Mittelalter die Sinne der Aerzte nicht überall durch
überlieferte Vorurtheile gefesselt wurden, sondern noch
mehr, dass der gesunde Menschenverstand im Volke
an gewissen Wahrheiten festgehalten hat, trotzdem dass
die gelehrte Kritik sie für überwunden erklärt. Was
sollte mich abhalten, zu gestehen, dass die gelehrte
Kritik nicht immer wahr, das System nicht immer
Natur gewesen ist, dass die falsche Deutung nicht die
Richtigkeit der Beobachtung beeinträchtigt? warum
sollte ich nicht gute Ausdrücke erhalten oder wiederherstellen,
trotzdem dass man falsche Vorstellungen
daran geknüpft hat? Meine Erfahrungen nöthigen mich,
die Bezeichnung der Wallung (Fluxion) für besser zu
halten, als die der Congestion; ich kann nicht umhin,
die Entzündung als eine bestimmte Erscheinungsform
[XIV] pathologischer Vorgänge zuzulassen, obwohl ich sie
als ontologischen Begriff auflöse; ich muss trotz des
entschiedenen Widerspruchs vieler Forscher den Tuberkel
als miliares Korn, das Epitheliom als heteroplastische,
maligne Neubildung (Cancroid) festhalten.
Vielleicht ist es in heutiger Zeit ein Verdienst,
das historische Recht anzuerkennen, denn es ist in
der That erstaunlich, mit welchem Leichtsinn gerade
diejenigen, welche jede Kleinigkeit, die sie gefunden
haben, als eine Entdeckung preisen, über die Vorfahren
aburtheilen. Ich halte auf mein Recht und darum erkenne
ich auch das Recht der Anderen an. Das ist
mein Standpunkt im Leben, in der Politik, in der
Wissenschaft. Wir sind es uns schuldig, unser Recht
zu vertheidigen, denn es ist die einzige Bürgschaft
unserer individuellen Entwickelung und unseres Einflusses
auf das Allgemeine. Eine solche Vertheidigung
ist keine That eitlen Ehrgeizes, kein Aufgeben
des rein wissenschaftlichen Strebens. Denn wenn wir
der Wissenschaft dienen wollen, so müssen wir sie
auch ausbreiten, nicht bloss in unserem eigenen Wissen,
sondern auch in der Schätzung der Anderen.
Diese Schätzung aber beruht zum grossen Theile auf
der Anerkennung, die unser Recht, auf dem Vertrauen,
das unsere Forschung bei den Anderen findet, und das
ist der Grund, warum ich auf mein Recht halte.
In einer so unmittelbar praktischen Wissenschaft,
wie die Medicin, in einer Zeit so schnellen Wachsens
der Erfahrungen, wie die unsrige, haben wir doppelt die
Verpflichtung, unsere Kenntniss der Gesammtheit der
Fachgenossen zugänglich zu machen. Wir wollen die
Reform, und nicht die Revolution. Wir wollen das Alte
conserviren und das Neue hinzufügen. Aber den Zeitgenossen
[XV] trübt sich das Bild dieser Thätigkeit. Denn nur
zu leicht gewinnt es den Anschein, als würde eben nur
ein buntes Durcheinander von Altem und Neuem gewonnen,
und die Notwendigkeit, die falschen oder
ausschliessenden Lehren der Neueren mehr, als die der
Alten zu bekämpfen, erzeugt den Eindruck einer mehr
revolutionären, als reformatorischen Einwirkung. Es
ist freilich bequemer, sich auf die Forschung und die
Wiedergabe des Gefundenen zu beschränken und Anderen
die “Verwerthung” zu überlassen, aber die Erfahrung
lehrt, dass dies überaus gefährlich ist und zuletzt
nur denjenigen zum Vortheil ausschlägt, deren
Gewissen am wenigsten zartfühlend ist. Uebernehmen
wir daher jeder selbst die Vermittelung zwischen der
Erfahrung und der Lehre.
Die Vorlesungen, welche ich hier mit der Absicht
einer solchen Vermittelung veröffentliche, haben so
ausdauernde Zuhörer gefunden, dass sie vielleicht auch
nachsichtige Leser erwarten dürfen. Wie sehr sie der
Nachsicht bedürfen, fühle ich selbst sehr lebhaft. Jede
Art von freiem Vortrage kann nur dem wirklichen Zuhörer
genügen. Zumal dann, wenn der Vortrag wesentlich
darauf berechnet ist, als Erläuterung für Tafel-Zeichnungen
und Demonstrationen zu dienen, muss er
nothwendig dem Leser ungleichmässig und lückenhaft
erscheinen. Die Absicht, eine gedrängte Uebersicht
zu liefern, schliesst an sich eine speciellere, durch ausreichende
Citate unterstützte Beweisführung mehr oder
weniger aus und die Person des Vortragenden wird
mehr in den Vordergrund treten, da er die Aufgabe
hat, gerade seinen Standpunkt deutlich zu machen.
Möge man daher das Gegebene für nicht mehr
nehmen, als es sein soll. Diejenigen, welche Musse
[XVI] genug gefunden haben, sich in der laufenden Kenntniss
der neueren Arbeiten zu erhalten, werden wenig Neues
darin finden. Die Anderen werden durch das Lesen
nicht der Mühe überhoben sein, in den histologischen,
physiologischen und pathologischen Specialwerken die
hier nur ganz kurz behandelten Gegenstände genauer
studiren zu müssen. Aber sie werden wenigstens eine
Uebersicht der für die cellulare Theorie wichtigsten
Entdeckungen gewinnen und mit Leichtigkeit das genauere
Studium des Einzelnen an die hier im Zusammenhange
gegebene Darstellung anknüpfen können.
Vielleicht wird gerade diese Darstellung einen unmittelbaren
Anreiz für ein solches genaueres Studium abgeben,
und schon dann wird sie genug geleistet haben.
Meine Zeit reicht nicht aus, um mir die schriftliche
Ausarbeitung eines solchen Werkes möglich zu
machen. Ich habe mich deshalb genöthigt gesehen,
die Vorlesungen, wie sie gehalten wurden, stenographiren
zu lassen und mit leichten Aenderungen zu
redigiren. Herr Cand. med. Langenhaun hat mit
grosser Sorgfalt die stenographische Arbeit besorgt.
Soweit es sich in der Kürze der Zeit thun liess, und
soweit der Text ohne dieselben für Ungeübte nicht
verständlich sein würde, habe ich nach den Tafel-Zeichnungen
und besonders nach den vorgelegten Präparaten
Holzschnitte anfertigen lassen; Vollständigkeit
liess sich in dieser Beziehung nicht erreichen, da schon
so die Veröffentlichung durch die Anfertigung der Holzschnitte
um Monate verzögert worden ist.
Misdroy, am 20. August 1858.
Rud. Virchow.
[Uebersicht der Holzsschnitte S. XVII–XXII.]
[1] Erste Vorlesung.
10. Februar 1858.
Einleitung und Aufgabe. Bedeutung der anatomischen Entdeckungen in der Geschichte der
Medicin. Geringer Einfluss der Zellentheorie auf die Pathologie. Die Zelle als letztes
wirkendes Element des lebenden Körpers. Genauere Bestimmung der Zelle. Die Pflanzenzelle:
Membran, Inhalt, Kern. Die thierische Zelle: die eingekapselte (Knorpel) und die
einfache. Der Zellenkern (Nucleus). Das Kernkörperchen (Nucleolus). Die Theorie der Zellenbildung
aus freiem Cytoblastem. Constanz des Kerns und Bedeutung desselben für die
Erhaltung der lebenden Elemente. Verschiedenartigkeit des Zelleninhalts und Bedeutung
desselben für die Function der Theile. Die Zellen als vitale Einheiten. Der Körper als
sociale Einrichtung. Die Cellularpathologie im Gegensatze zur Humoral- und
Solidarpathologie.
Erläuterung einiger Präparate. Junge Pflanzentriebe. Pflanzenwachsthum. Knorpelwachsthum.
Junge Eierstockseier. Junge Zellen im Auswurf.
Meine Herren, indem ich Sie herzlich willkommen heisse
auf Bänken, die Ihnen seit Langem ungewohnt sein werden,
so muss ich im Voraus bemerken, dass es nicht meine Unbescheidenheit
ist, welche Sie hierher berufen hat, sondern dass
ich nur dem wiederholt ausgesprochenen Wunsche vieler unter
Ihnen nachgegeben habe. Auch würde ich es nicht gewagt
haben, Ihnen Vorträge in der Weise anzubieten, wie ich sie
in meinen regelmässigen Cursen zu halten pflege, vielmehr
will ich den Versuch machen, in etwas mehr zusammenfassender
Art Ihnen die Entwicklung vorzuführen, welche ich selbst,
und, wie ich denke, welche auch die medicinische Wissenschaft im
Verlaufe der letzten Decennien gemacht hat. Schon in der
Ankündigung habe ich die Vorlesungen so bezeichnet, dass
ich neben die Pathologie die Histologie gestellt habe, aus
dem Grunde, weil ich voraussetzen zu müssen glaube, dass
[2] vielen unter Ihnen, welchen vielleicht die neuesten histologischen
Wechsel nicht ganz geläufig sind, eigene Anschauungen
mikroskopischer Dinge nicht hinreichend zu Gebote stehen.
Da jedoch gerade auf solche Anschauungen die wichtigen
Schlüsse sich stützen, die wir gegenwärtig ziehen, so
werden Sie es verzeihen, wenn ich, ohne Rücksicht auf
diejenigen unter Ihnen, welche vollständig orientirt sind, mich
so anstelle, als ob Sie alle nicht ganz in den nöthigen
Vorkenntnissen zu Hause wären.
Die gegenwärtige Reform der Medicin, die Sie alle mit erlebt
haben, ging wesentlich aus von neuen anatomischen Erfahrungen,
und auch das, was ich Ihnen vorzutragen habe, soll sich vorzüglich
auf anatomische Demonstrationen stützen. Aber es würde
für mich nicht ausreichen, wie es in dem letzten Jahrzehnt
gebräuchlich war, nur die pathologische Anatomie als Grundlage
der Anschauung zu nehmen; wir müssen auch die
allgemein-anatomischen Thatsachen hinzufügen, aus welchen die
augenblickliche Gestaltung der Wissenschaft gewonnen worden
ist. Die Geschichte der Medicin lehrt uns ja, wenn wir
nur einen einigermassen grosseren Ueberblick nehmen, dass zu
allen Zeiten die eigentlichen Fortschritte bezeichnet worden
sind durch anatomische Neuerungen, und dass jede grössere Phase
der Entwicklung zunächst eingeleitet worden ist durch eine Reihe
von bedeutenden Entdeckungen über den Bau des Körpers.
So ist es in der alten Zeit gewesen, als die Erfahrungen der
Alexandriner, zum ersten Male von der Anatomie des Menschen
ausgehend, das galenische System vorbereiteten, so im Mittelalter,
als Vesal wiederum die Anatomie neu begründete und
damit die eigentliche Reform der Medicin begann, so endlich, als
Bichat die Grundsätze der allgemeinen Anatomie entwickelte.
Dasjenige, was Schwann gethan hat für die Gewebelehre,
das ist für die Pathologie bis jetzt sehr wenig ausgebaut
und entwickelt worden, und man kann sagen, dass nichts weniger
in das allgemeine Bewusstsein eingedrungen ist, als die
Zellentheorie in ihrer nahen Beziehung zur Pathologie.
Wenn man den ausserordentlichen Einfluss erwägt, welchen
seiner Zeit Bichat auf die Gestaltung der ärztlichen
Anschauungen ausgeübt hat, so ist es in der That erstaunlich,
[3] dass eine so verhältnissmässig lange Zeit vergangen ist, seitdem
Schwann seine grossen Entdeckungen machte, ohne dass
man die eigentliche Breite der neuen Thatsachen würdigte.
Es hat dies allerdings sehr wesentlich an der immer noch
unvollständigen Kenntniss der feineren Einrichtung unserer Gewebe
gelegen, welche bis in die neueste Zeit bestanden hat, und
welche, wie wir leider zugestehen müssen, in manchen Theilen
der Histologie selbst jetzt noch in solchem Maasse herrscht,
dass man kaum weiss, für welche Ansicht man sich
entscheiden soll.
Besondere Schwierigkeiten hat die Beantwortung der
Frage gemacht, von welchen Theilen des Körpers eigentlich
die Action ausgeht, welcher Theil thätig, welcher leidend ist;
doch ist ein Abschluss darüber schon jetzt in der That vollständig
möglich, selbst bei solchen Theilen, über deren Struktur
noch gestritten wird. Es handelt sich bei dieser Anwendung
der Histologie auf Physiologie und Pathologie zunächst
um die Anerkennung, dass die Zelle wirklich das letzte eigentliche
Form-Element aller lebendigen Erscheinung sei, und
dass wir die eigentliche Action nicht über die Zelle hinausverlegen
dürfen. Ihnen gegenüber werde ich mich nicht besonders
zu rechtfertigen haben, wenn ich in dieser Beziehung
etwas ganz Besonderes dem Leben vorbehalte. In der Folge
dieser Vorträge werden Sie sich überzeugen, dass man für
das Einzelne kaum mechanischer denken kann, als ich es zu
thun pflege, wo es sich darum handelt, Vorgänge, deren
Erklärung wir suchen, zu deuten. Aber ich glaube, dass man
das festhalten muss, dass, wie viel auch von dem feineren
Stoff-Verkehr, der innerhalb der Zelle geschieht, jenseits des
materiellen Gebildes als Ganzen liegen mag, doch die eigentliche
Action von diesem Gebilde als solchem ausgehe, und dass das
lebende Element nur so lange wirksam ist, als es uns wirklich
als Ganzes, für sich bestehend, entgegentritt.
In dieser Frage kommt es zunächst darauf an, und Sie
werden mir verzeihen, wenn ich dabei etwas verweile, weil dies
ein Punkt ist, welcher noch jetzt streitig ist, dass wir feststellen,
was man eigentlich unter einer Zelle zu verstehen habe.
Gleich im Anfang, als die neueste Phase der histologischen
[4] Entwicklung begonnen wurde, häuften sich grosse Schwierigkeiten,
indem, wie Ihnen bekannt sein wird, Schwann, zunächst
auf den Schultern von Schleiden stehend, seine Beobachtungen
nach botanischen Mustern deutete, so dass alle Lehrsätze
der Pflanzen-Physiologie in einem nicht unerheblichen Maasse
entscheidend wurden für die Physiologie der thierischen Körper.
Die Pflanzenzelle in dem Sinne, wie man sie zu jener
Zeit ganz allgemein fasste, und wie sie auch gegenwärtig
häufig noch gefasst wird, ist aber ein Gebilde, dessen Identität
mit dem, was wir thierische Zelle nennen, nicht ohne Weiteres
zugestanden werden kann.
Wenn man von gewöhnlichem Pflanzenzellgewebe spricht,
so meint man im Allgemeinen damit ein Gewebe, das in seiner
einfachsten und regelmässigsten Form auf einem Querschnitt
(Fig. 1. a.) aus lauter vier- oder sechseckigen, wenn es etwas
loser ist, aus rundlichen oder polygonalen Körpern besteht, an
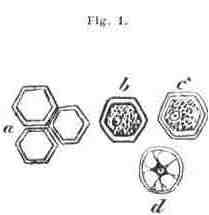 |
denen man stets eine ziemlich dicke, derbe Wand (Membran) unterscheidet. Isolirt man einen einzelnen solchen Körper, so findet man einen Hohlraum, umgeben von dieser derben, eckigen oder runden Wand, in dessen Innerem je nach Umständen sehr verschiedene Stoffe abgelagert sein können, z.B. Fett, Stärke, Pigment, Eiweiss (Zelleninhalt). |
Es hat sich frühzeitig herausgestellt, dass, ganz
abgesehen von diesen örtlichen Verschiedenheiten des Inhaltes,
[5] die chemische Untersuchung an den zelligen Elementen mehrere
verschiedene Stoffe nachzuweisen im Stande ist.
Die Substanz, welche die äussere Membran bildet, und welche
unter dem Namen der Cellulose bekannt ist, zeigt sich im Allgemeinen
als stickstofflos, und gibt die eigenthümliche, sehr
charakteristische, schön blaue Färbung bei Zusatz von Jod
und Schwefelsäure. (Jod allein gibt keine Färbung, die
Schwefelsäure für sich verkohlt.) Der Inhalt der Zellen dagegen
wird nicht blau; wenn die Zelle recht einfach ist, so tritt
vielmehr durch die Einwirkung von Jod und Schwefelsäure
eine bräunliche oder gelbliche Masse hervor, die sich als besonderer
Körper im Inneren des Zellenraumes isolirt (Protoplasma)
und an der sich eine zweite, faltige, häufig geschrumpfte
Haut (Primordialschlauch) erkennen lässt (Fig. 1. c.).
Auch die gröbere chemische Analyse zeigt an den einfachsten
Zellen gewöhnlich neben der stickstofflosen (äusseren) Substanz
eine stickstoffhaltige (Inhalts-)Masse, und die Pflanzen-Physiologie
hatte somit ein Recht zu schliessen, dass das
eigentliche Wesen einer Zelle darin beruhe, dass innerhalb einer
stickstofflosen Membran ein von ihr differenter stickstoffhaltiger
Inhalt vorhanden sei.
Man wusste freilich schon seit längerer Zeit, dass noch andere
Dinge sich im Innern der Zellen befinden, und es war eine
der folgenreichsten Entdeckungen, als Rob. Brown den Kern
(Nucleus) innerhalb der Zelle entdeckte. Aber man legte diesem
Gebilde eine grössere Bedeutung für die Bildung als für
die Erhaltung der Zellen bei, weil in sehr vielen Pflanzenzellen
der Kern äusserst undeutlich wird, in vielen ganz verschwindet,
während die Form der Zelle erhalten bleibt.
Mit solchen Erfahrungen kam man an die thierischen Gewebe,
deren Uebereinstimmung mit den pflanzlichen Schwann
nachzuweisen suchte. Die eben besprochene Deutung der
gewöhnlichen pflanzlichen Zellenform diente als Ausgangspunkt.
Dies ist aber, wie die spätere Erfahrung gezeigt hat, in gewissem
Sinne irrig gewesen. Man kann die pflanzliche Zelle
in ihrer Totalität nicht mit jeder beliebigen thierischen zusammenstellen.
Wir kennen an thierischen Zellen keine solche
Differenzen zwischen stickstoffhaltigen und stickstofflosen
[6] Schichten; in allen wesentlich die Zelle constituirenden
Theilen kommen stickstoffhaltige Materien vor. Aber es
gibt allerdings gewisse Formen im thierischen Leibe, welche
an diese Formen der pflanzlichen Zellen unmittelbar erinnern,
und unter diesen ist keine so charakterisch als die Zellenformation
im Knorpel, der seiner ganzen Erscheinung nach
von den übrigen Geweben des thierischen Leibes äusserst verschieden
ist, und der namentlich durch seine Gefässlosigkeit eine
besondere Stellung einnimmt. Der Knorpel schliesst sich unmittelbar
durch die Eigenthümlichkeit seiner Elemente an die
Pflanze an. An einer recht entwickelten Knorpelzelle erkennen
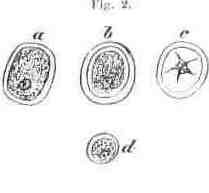 |
wir eine verhältnissmässig dicke äussere Schicht, innerhalb welcher, wenn wir recht genau zusehen, wiederum eine zarte Haut, ein Inhalt, und ein Kern zu finden sind. Hier haben wir allerdings ein Gebilde, das der Pflanzenzelle durchaus entspricht. |
Man hat aber gewöhnlich, wenn man den Knorpel schilderte,
das ganze eben beschriebene Ding (Fig. 2. a-d) ein Knorpelkörperchen
genannt, und indem man dasselbe als analog den Zellen
anderer thierischer Theile auffasste, so ist man in Schwierigkeiten
gerathen, welche die Kenntniss des wahren Sachverhältnisses
ungemein störten. Das Knorpelkörperchen ist nehmlich
nicht als Ganzes eine Zelle, sondern die äussere Schicht,
die Capsel, ist das Produkt einer späteren Entwicklung (Absonderung,
Ausscheidung). Im jungen Knorpel ist sie sehr
dünn, während auch die Zelle kleiner zu sein pflegt. Gehen
wir noch weiter in der Entwickelung zurück, so treffen wir
auch im Knorpel nichts als die einfache Zelle, dasselbe Gebilde,
welches auch sonst in thierischen Gebilden vorkommt,
und das jene äussere Absonderungsschicht nicht besitzt.
Sie sehen daraus, meine Herren, dass die Vergleichung
[7] zwischen thierischen und pflanzlichen Zellen, die wir allerdings
machen müssen, insofern unzulässig ist, als in den meisten
thierischen Geweben keine Formelemente gefunden werden, die
als Aequivalente der Pflanzenzelle in der alten Bedeutung dieses
Wortes betrachtet werden können, dass insbesondere die
Cellulose-Membran der Pflanzenzelle nicht der thierischen Zellhaut
entspricht, und dass die letztere als stickstoffhaltig nicht
eine typische Verschiedenheit von der ersteren als stickstofflosen
darbietet. Vielmehr treffen wir in beiden Fällen eine
Bildung, die wesentlich stickstoffhaltiger Natur und im Grossen
von übereinstimmender Zusammensetzung ist. Die sogenannte
Membran der Pflanzenzelle findet sich nur in einigen thierischen
Gebilden, z.B. im Knorpel wieder; die gewöhnliche
Membran der Thierzelle entspricht dem Primordialschlauch der
Pflanzenzelle. Erst wenn man diesen Standpunkt festhält,
wenn man von der Zelle Alles ablöst, was durch eine spätere
Entwicklung hinzugekommen ist, so gewinnt man ein einfaches,
gleichartiges, äusserst monotones Gebilde, welches sich mit
ausserordentlicher Constanz in den lebendigen Organismen wiederholt.
Aber gerade diese Constanz ist das beste Kriterium
dafür, dass wir in ihm das eigentlich Elementare haben, welches
alles Lebendige charakterisirt, ohne dessen Präexistenz
keine lebendigen Formen entstellen, und an welches der eigentliche
Fortgang, die Erhaltung des Lebens gebunden ist. Erst
seitdem der Begriff der Zelle diese strenge Form angenommen
hat, und ich bilde mir etwas darauf ein, trotz des Vorwurfes
der Pedanterie stets daran festgehalten zu haben, erst seit dieser
Zeit kann man sagen, dass eine einfache Form gewonnen
ist, die wir überall wieder aufsuchen können, und die, wenn
auch in Grösse und äusserer Gestaltung verschieden, doch in
ihren wesentlichen Bestandtheilen immer gleichartig ist.
An einer solchen einfachen Zelle unterscheiden wir ziemlich
verschiedenartige Bestandtheile, und es ist wichtig, dass
wir auch diese genau auseinanderlegen.
Zuerst erwarten wir, dass innerhalb der Zelle ein Kern
sei. Von diesem Kerne, der in der Regel eine ovale oder
runde Form hat, wissen wir, dass er, zumal in jungen Elementen
eine grössere Resistenz gegen chemische Einwirkungen
[8] 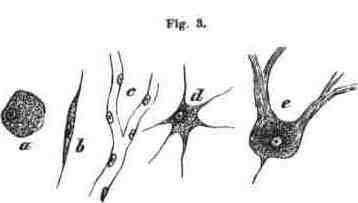
besitze, als die äusseren Theile der Zelle, und dass er trotz
der grössten Variabilität der äusseren Gestalt der Zelle seine
Gestalt im Allgemeinen behaupte. Der Kern ist demnach derjenige
Theil der Zelle, der mit grosser Constanz in allen Formen
unverändert wiederkehrt. Freilich gibt es einzelne Fälle,
welche durch die ganze Reihe der vergleichend-anatomischen
und pathologischen Thatsachen zerstreut liegen, in denen auch
der Kern zackig oder eckig erscheint, aber dies sind ganz seltene
Ausnahmen, gebunden an besondere Veränderungen, welche
das Element eingegangen ist. Im Allgemeinen kann
man sagen, dass so lange als es noch zu keinem Abschluss
des Zellenlebens gekommen ist, so lange als die Zellen sich
als lebenskräftige Elemente verhalten, die Kerne eine nahezu
constante Form besitzen.
Der Kern seinerseits enthält bei entwickelten Elementen
wiederum mit grosser Beständigkeit ein Gebilde in sich, das
sogenannte Kernkörperchen (Nucleolus). In Beziehung auf
die Frage von der vitalen Form kann man von dem Nucleolus
nicht sagen, dass er als ein nothwendiges Desiderat erscheine;
in einer erheblichen Zahl von jungen Elementen ist
es noch nicht gelungen, ihn zu sehen. Dagegen treffen wir
ihn bei ganz entwickelten älteren Formen regelmässig, und
er scheint daher eine höhere Ausbildung des Elementes anzuzeigen.
Nach der Aufstellung, welche ursprünglich von Schleiden
gemacht, von Schwann acceptirt wurde, dachte man
sich lange Zeit das Verhältniss der drei coexistenten Zellentheile
so, dass der Nucleolus bei der Entwickelung der Gewebe als
[9] das Erste aufträte, indem er sich aus einer Bildungsflüssigkeit
(Blastem, Cytoblastem) ausscheide, dass er schnell eine
gewisse Grösse erreiche, dass sich dann um ihn kleine Körnchen
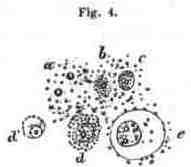 |
aus dem Blastem niederschlügen, um die sich eine Membran verdichte; damit wäre ein Nucleus fertig, um den sich nun allmählich neue Masse ansammle und seiner Zeit eine kleine Membran erzeuge (die berühmte Uhrglasform.) Diese |
Darstellung der ersten Entwicklung von Zellen aus freiem Blastem,
wonach der Kern der Zellenbildung voraufgehen und als
eigentlicher Zellenbildner (Cytoblast) auftreten sollte, ist es,
welche man gewöhnlich unter dem Namen der Zellentheorie
(genauer Theorie der freien Zellenbildung) zusammenzufassen
pflegt, – eine Theorie der Entwicklung, welche fast vollständig
verlassen ist, und für deren Richtigkeit keine einzige Thatsache
mit Sicherheit beigebracht werden kann. In Beziehung auf
das Kernkörperchen ist vorläufig nur das festzuhalten, dass,
wenn wir entwickelte, grosse Zellen haben, wir fast constant
auch einen Nucleolus in ihnen sehen, dass dagegen bei vielen
jungen Elementen derselbe vermisst wird.
Sie werden späterhin eine Reihe von Thatsachen
der pathologischen und physiologischen Entwicklungsgeschichte
kennen lernen, welche es in hohem Grade wahrscheinlich
machen, dass der Kern eine ausserordentlich wichtige Rolle
innerhalb der Zelle spielt, eine Rolle, die, wie ich gleich hervorheben
will, weniger auf die Function, die specifische Leistung
der Elemente sich bezieht, als vielmehr auf die Erhaltung
und Vermehrung des Elementes als eines lebendigen
[10] Theiles. Die specifische (im engern Sinne animalische) Function
zeigt sich am deutlichsten am Muskel, am Nerven, an der
Drüsenzelle; ihre besonderen Thätigkeiten der Contraction, der
Sensation, der Secretion, scheinen in keiner unmittelbaren
Weise mit den Kernen etwas zu thun zu haben. Aber dass
inmitten aller Function das Element ein Element bleibt, dass
es nicht vernichtet wird und zu Grunde geht unter der fortdauernden
Thätigkeit, dies scheint wesentlich an die Thätigkeit
des Kerns gebunden zu sein. Alle diejenigen zelligen
Bildungen, welche ihren Kern verlieren, sehen wir mehr transitorisch
zu Grunde gehen, sie verschwinden, sterben ab, lösen
sich auf. Ein menschliches Blutkörperchen z.B. ist eine Zelle
ohne Kern; es besitzt eine äussere Membran und einen rothen
Inhalt, aber damit ist seine Zusammensetzung, so weit man
sie erkennen kann, erschöpft, und was man vom Blutkörperchen-Kern
beim Menschen erzählt hat, bezieht sich auf Täuschungen,
welche allerdings sehr leicht und häufig hervorgebracht
werden dadurch, dass kleine Unebenheiten der Oberfläche
sich bilden. Man könnte daher nicht sagen, dass Blutkörperchen
Zellen seien, wenn wir nicht wüssten, dass eine
gewisse Zeit existirt, wo auch die menschlichen Blutkörperchen
Kerne haben, nehmlich die Zeit innerhalb der ersten
Monate des intrauterinen Lebens. Hier cursiren auch beim
Menschen kernhaltige Blutkörperchen, wie man sie bei Fröschen,
Vögeln, Fischen das ganze Leben hindurch sieht. Das
ist bei Säugethieren auf eine gewisse Zeit der Entwicklung
beschränkt, so dass in der späteren Zeit die rothen
Blutkörperchen nicht mehr die volle Zellennatur an sich tragen,
sondern einen wichtigen Bestandtheil ihrer Zusammensetzung
eingebüsst haben. Aber wir alle sind auch darüber
einig, dass gerade das Blut eines von den wechselnden Bestandtheilen
des Körpers ist, die keine Dauerhaftigkeit der Elemente
besitzen, von denen Jeder annimmt, dass ihre Theile
zu Grunde gehen und ersetzt werden durch neue, die wiederum
der Vernichtung bestimmt sind, und die überall (wie
die obersten Epidermiszellen, in welchen wir auch keine Kerne
finden, so bald sie sich abschilfern) schon ein Stadium ihrer
Entwicklung erreicht haben, wo sie nicht mehr jener Dauerhaftigkeit
[11] der innereren Zusammensetzung bedürfen, als deren
Bürgen wir den Kern betrachten müssen.
Dagegen kennen wir, so vielfach auch gegenwärtig die
Gewebe untersucht sind, keinen Theil, der wächst, der sich
vermehrt, sei es physiologisch oder pathologisch, wo nicht mit
Nothwendigkeit kernhaltige Elemente als die Ausgangspunkte
der Veränderung nachweisbar wären, und wo nicht die ersten
entschiedenen Veränderungen, welche auftreten, den Kern selbst
betreffen, so dass wir aus seinem Verhalten oft bestimmen können,
was möglicher Weise aus den Elementen geworden sein würde.
Sie sehen nach dieser Darstellung, dass wenigstens zweierlei
für die Zusammensetzung eines zelligen Elementes als
nothwendiges Desiderat verlangt werden muss, nämlich die
Membran, mag sie nun rund oder zackig oder sternförmig
sein, und der Kern, welcher von vorn herein eine andere
chemische Beschaffenheit besitzt als die Membran. Es ist indess
damit lange nicht alles Wesentliche erschöpft, denn die
Zelle ist ausser dem Kern gefüllt mit einer verhältnissmässig
grösseren oder kleineren Menge von Inhaltsmasse, und ebenso
in der Regel, wie es scheint, der Kern seinerseits, in der Art,
 |
dass der Inhalt des Kerns wieder verschieden zu sein pflegt von dem Inhalte der Zelle. Innerhalb der Zelle z.B. sehen wir Pigment, ohne dass der Kern etwas davon enthielte. Innerhalb einer glatten Muskelzelle wird die contractile Substanz abgelagert, welche als Trägerin der contractilen Kraft der Muskeln erscheint; der Kern aber bleibt Kern. Das zellige Element kann sich zu einer Nervenfaser entwickeln, aber der Kern bleibt ausserhalb des Markes als constantes Gebilde liegen. Daraus geht hervor, dass die besonderen Eigenthümlichkeiten, welche die einzelnen Zellen an besonderen Orten unter besonderen Bedingungen erreichen, im Allgemeinen gebunden sind an wechselnde |
[12] Eigenschaften des Zelleninhalts, dass es nicht die bisjetzt betrachteten
Bestandtheile (Membran und Kern), sondern der Inhalt
oder auch ausserhalb der Zelle abgelagerte Massen sind, welche
die functionelle (physiologische) Verschiedenheit der Gewebe
bedingen. Für uns ist es wesentlich zu wissen, dass
innerhalb der verschiedensten Gewebe jene Bestandtheile, welche
die Zelle gewissermaassen in ihrer abstracten Form darstellen,
Kern und Membran, mit grosser Beständigkeit wiederkehren,
und dass durch ihre Zusammenfügung ein einfaches
Element gewonnen wird, welches durch die ganze Reihe der
lebendigen pflanzlichen und thierischen Gestaltungen, so äusserlich
verschieden sie auch sein mögen, so sehr die innere
Zusammensetzung dem Wechsel unterworfen sein mag, eine
ganz besondere Formbildung als bestimmte Grundlage aller
Lebenserscheinungen erkennen lässt.
Meiner Auffassung nach ist dies der einzig mögliche Ausgangspunkt
aller biologischen Doctrinen. Wenn eine bestimmte
Uebereinstimmnng der elementaren Form durch die ganze
Reihe alles Lebendigen hindurchgeht, und wenn man vergeblich
in dieser Reihe nach irgend etwas Anderem sucht, was
an die Stelle der Zelle gesetzt werden könnte, so muss man
nothwendig auch jede höhere Ausbildung, sei es einer Pflanze
oder eines Thieres, zunächst betrachten als eine progressive
Summirung einer grösseren oder kleineren Zahl gleichartiger
oder ungleichartiger Zellen. Wie ein Baum eine in einer bestimmten
Weise zusammengeordnete Masse darstellt, in welcher
als letzte Elemente an jedem einzelnen Theile, am Blatt
wie an der Wurzel, am Stamm wie an der Blüthe, zellige Elemente
erscheinen, so ist es auch mit den thierischen Gestalten.
Jedes Thier erscheint als eine Summe vitaler Einhei-
ten, von denen jede den vollen Charakter des Lebens an
sich trägt. Der Charakter und die Einheit des Lebens kann
nicht an einem bestimmten Punkte einer höheren Organisation
gefunden werden, z. B. im Gehirn des Menschen, sondern nur
in der bestimmten, constant wiederkehrenden Einrichtung, welche
jedes einzelne Element an sich trägt. Daraus geht hervor, dass
die Zusammensetzung eines grösseren Körpers immer auf eine
[13] Art von gesellschaftlicher Einrichtung herauskommt, eine Einrichtung
socialer Art, wo eine Masse von einzelnen Existenzen
auf einander angewiesen ist, aber so, dass jedes Element für
sich eine besondere Thätigkeit hat, und dass jedes, wenn es
auch die Anregung zu seiner Thätigkeit von anderen Theilen
her empfängt, doch die eigentliche Leistung von sich ausgehen
lässt.
Ich habe es deshalb für nothwendig erachtet, und ich glaube,
dass Sie Nutzen davon haben werden, den Körper zu zerlegen
in Zellenterritorien. Ich habe gesagt Territorien, weil wir
in der thierischen Organisation eine Eigenthümlichkeit finden,
welche in der Pflanze fast gar nicht zur Anschauung kommt,
nämlich die Entwicklung grosser Massen sogenannten intercellularen
Gewebes. Während die Pflanzenzellen in der
Regel mit ihren äusseren Absonderungsschichten unmittelbar
aneinander stossen, so jedoch, dass man immer noch die alten
Grenzen unterscheiden kann, so finden wir bei den thierischen
Geweben, dass diese Art der Anordnung die seltnere
ist. Hier treffen wir eine oft sehr reichliche Masse zwischen
den Zellen (Zwischensubstanz, Intercellularsubstanz),
aber wir können selten von vornherein Übersehen, inwieweit
[14] ein bestimmter Theil davon der einen, ein anderer der anderen
Zelle angehöre.
Nach Schwann war die Intercellularsubstanz eine Art
von Cytoblastem, für die Entwicklung neuer Zellen bestimmt.
Dies halte ich nicht für richtig, vielmehr bin ich durch eine
Reihe von pathologischen Erfahrungen dahin gekommen, einzusehen,
dass die Intercellularsubstanz in einer bestimmten Abhängigkeit
von den Zellen sich befindet und dass es nothwendig ist,
auch in ihr Grenzen zu ziehen und zuzugestehen, dass
auch von der Intercellularsubstanz gewisse Bezirke der einen
und gewisse der andern Zelle angehören. Sie werden sehen,
wie pathologische Vorgänge diese Grenzen scharf markiren,
wie sich direkt zeigen lässt, dass ein bestimmtes Territorium
von Zwischensubstanz beherrscht wird von einem Zellen-Elemente,
welches in dessen Mitte gelegt ist und von welchem
Wirkungen auf die Nachbarschaft ausgehen.
Es wird jetzt deutlich sein, wie ich mir die Zellen-Territorien
denke: Es gibt Gewebe, welche ganz aus Zellen bestehen,
Zelle an Zelle gelagert. Hier kann über die Grenze
der einzelnen Zelle keine Schwierigkeit bestehen, aber es ist nöthig,
hervorzuheben, dass auch in diesem Falle jede einzelne Zelle
ihre besonderen Wege gehen, ihre besonderen Veränderungen er-
fahren kann, ohne dass mit Notwendigkeit das Geschick der zunächstliegenden
Zelle daran geknüpft ist. In andern Geweben
dagegen, wo wir Zwischenmassen haben, versorgt die Zelle
ausser ihrem eignen Inhalt noch eine gewisse Menge von
äusserer Substanz, die mit au ihren Veränderungen Theil
nimmt, ja sogar häufig frühzeitiger afficirt wird, als das Innere der
Zelle, welches mehr gesichert ist durch seine Lagerung als die
äussere Zwischenmasse. Endlich gibt es eine dritte Reihe
von Geweben, deren Elemente untereinander in engeren Verbindungen
stehn. Es kann z. B. eine sternförmige Zelle mit
einer ähnlichen zusammenhängen, und dadurch eine netzförmige
Anordnung entstehen, ähnlich derbei denCapillaren und anderen
analogen Gebilden. In diesem Falle könnte man glauben,
dass die ganze Reihe beherrscht werde von irgend Etwas, was
wer weiss wie weit entfernt liegt, indessen bei genauerem
Studium ergibt sich, dass selbst in diesen kettenartigen Elementen
[15] eine gewisse Unabhängigkeit der einzelnen Glieder
besteht, und dass diese Unabhängigkeit sich äussert, indem
unter gewissen äusseren oder inneren Einwirkungen das Element
nur innerhalb seiner Grenzen gewisse Veränderungen erfährt,
ohne dass die nächsten Elemente dabei betheiligt zu sein
brauchen.
Das Angeführte wird zunächst genügen, um Ihnen zu zeigen,
in welcher Weise ich es für nothwendig erachte, die pathologischen
Erfahrungen auf bekannte histologische Elemente
zurückzuführen, warum es mir nicht genügt z. B. von einer
Thätigkeit der Gefässe zu sprechen oder von einer Thätigkeit
der Nerven, sondern warum ich es für nothwendig erachte,
neben Gefässen und Nerven die grosse Zahl von kleinen
Theilen ins Auge zu fassen, welche eigentlich die Hauptmasse
der Körpersubstanz ausmachen. Es genügt nicht, dass man,
wie es seit langer Zeit geschieht, die Muskeln als thätige
Elemente daraus ablöst; innerhalb des grossen Restes, der gewöhnlich
als eine träge Masse betrachtet wird, findet sich
noch eine ungeheure Zahl wirksanier Theile.
In der Entwicklung, welche die Medicin bis in die letzte
Zeit genommen hat, finden wir den Streit zwischen den humoralen
und solidaren Schulen der alten Zeit immer noch erhalten.
Die humoralen Schulen haben im Allgemeinen das
meiste Glück gehabt, weil sie die bequemste Erklärung und
in der That die plausibelste Deutung der Krankheitsvorgänge
gebracht haben. Man kann sagen, dass fast alle glücklichen
Praktiker und bedeutenden Kliniker mehr oder weniger humoralpathologische
Tendenzen gehabt haben; ja diese sind so
populär geworden, dass es jedem Einzelnen äusserst schwer
wird, sich aus ihnen zu befreien. Die solidarpathologischen
Ansichten sind mehr eine Liebhaberei speculativer Forscher
gewesen und nicht sowohl aus dem unmittelbaren pathologischen
Bedürfnisse, als vielmehr aus physiologischen und philosophischen,
selbst aus religiösen Speculationen hervorgegangen.
Sie haben den Thatsachen Gewalt anthun müssen, sowohl in
der Anatomie als in der Physiologie, und haben daher nie-
mals eine ausgedehnte Verbreitung gefunden. Meiner Auffassung
nach ist der Standpunkt beider Lehren ein unvollständiger;
[16] ich sage nicht ein falscher, weil er eben nur falsch
ist in seiner Exclusion; er muss zurückgeführt werden auf
gewisse Grenzen, und man muss sich erinnern, dass neben
Gelassen und Blut, neben Nerven und Centralapparaten noch
andere Dinge existiren, die nicht ein blosses Substrat der
Einwirkung von Nerven und Blut sind, auf welchem diese
ihr Wesen treiben.
Wenn man nun fordert, dass die medicinischen Anschauungen
auch auf dieses Gebiet sich übertragen sollen,
wenn man andererseits verlangt, dass auch innerhalb der
humoral- und neuropathologischen Vorstellungen man sich
schliesslich erinnern soll, dass das Blut aus vielen
einzelnen für sich bestehenden Theilen besteht, dass das
Nervensystem aus vielen Sonderbestandtheilen zusammengesetzt
ist, so ist dies eine Forderung, die freilich auf den
ersten Blick manche Schwierigkeiten bietet. Aber wenn Sie
sich erinnern, dass man Jahre lang nicht bloss in den Vorlesungen,
sondern auch am Krankenbette von der Thätigkeit
der Capillaren gesprochen hat, einer Thätigkeit, die
Niemand gesehen hat, die eben nur auf bestimmte Doctrinen
hin angenommen worden ist, so werden Sie es nicht
unbillig finden, dass Dinge, die wirklich zu sehen sind, ja
die, wenn man sich übt, selbst dem unbewaffneten Auge
uicht selten zugängig sind, gleichfalls in den Kreis des
ärztlichen Wissens und Denkens aufgenommen werden. Von
Nerven hat man nicht nur gesprochen, wo sie nicht dargestellt
waren, man hat sie einfach supponirt, selbst in
Theilen, wo bei den sorgfältigsten Untersuchungen sich
nichts von ihnen hat nachweisen lassen; man hat sie wirksam
sein lassen an Punkten, wohin sie überhaupt gar nicht
vordringen. So ist es denn gewiss eine billige Forderung,
dass dem grösseren Theile des Körpers eine gewisse Anerkennung
werde, und wenn diese Anerkennung zugestanden
wird, dass man sich nicht mehr mit der blossen Ansicht
der Nerven als ganzer Theile, als eines zusammenhängenden
einfachen Apparates, oder des Blutes als eines blos flüssigen
Stoffes begnüge, sondern dass man auch innerhalb des Blutes
[17] und des Nervenapparates eine Masse wirksamer kleiner
Centren zulasse.
———————
Zum Schlüsse habe ich noch einige Präparate zu erläutern:
Ich fange mit einem sehr gewöhnlichen Objecte
an. Es ist von einem Kartoffelknollen hergenommen, an einer
Stelle, wo Sie die vollkommene Structur einer Pflanzenzelle
übersehen können: da, wo der Knollen anfängt, einen neuen
Schoss zu treiben, wo also die Wahrscheinlichkeit besteht,
dass man junge Zellen finden wird, vorausgesetzt, dass das
Wachsthum überhaupt in der Entwicklung neuer Zellen besteht.
Im Innern des Knollens sind bekanntlich alle Zellen
mit Amylonkörpern vollgestopft; an dem jungen Schoss dagegen
wird in dem Maasse, als er wächst, das Amylon
verbraucht, und die Zelle zeigt sich wieder in ihrer reineren
Gestalt. Auf einem Querschnitte durch einen jungen
Schössling nahe an seinem Austritte aus dem Knollen unterscheidet
man etwa vier verschiedene Lagen: die Rindenschicht,
dann eine Schicht grösserer Zellen, dann eine Schicht
kleinerer Zellen, und zuinnerst wieder eine Lage von grösseren.
Hier sieht man lauter regelmässige Gebilde; dicke Kapseln
von sechseckiger Gestalt, und im Innern derselben einen oder
ein Paar Kerne (Fig. l). Gegen die Rinde (Kork Schicht) hin
sind die Zellen viereckig und je weiter nach aussen, um so
 |
platter, aber auch in ihnen erkennt man bestimmt Kerne. Ueberall, wo die sogenannten Zellen zusammenstossen, ist zwischen ihnen eine Scheidegrenze zu erkennen; dann kommt die dicke Celluloseschicht, in welcher feine Streifen zu erkennen sind, und im Innern der Höhle sehen Sie eine zusammengesetzte Masse, in welcher |
[18] leicht ein Kern mit Kernkörperchen zu unterscheiden ist,
und in der nach Anwendung von Reagentien auch der
Primordialschlauch (Utriculus) als eine gefaltete, runzlige
Haut zum Vorschein kommt. Es ist dies die vollendete
Form der Pflanzenzelle. In den benachbarten Zellen liegen
einzelne grössere, matt glänzende, geschichtete Körper: die
Reste von Stärkemehl. – Das folgende Object ist mir deshalb
von Bedeutung, weil ich später darauf Bezug zu nehmen
habe beim Vergleich mit thierischen Neubildungen. Es
ist ein Längsschnitt aus der jungen Knospe eines Ligustrum-Strauches,
wie ihn die warmen Tage des Februar entwickelt
haben. In der Knospe sind schon eine Menge von jungen
Trieben angelegt, jeder aus zahlreichen jungen Zellen zusammengesetzt.
 |
In diesen jüngsten Theilen bestehen die äussern Schichten aus ziemlich regelmässigen Zellenlagen, die mehr platt viereckig erscheinen, während in den inneren Lagen die Zellen mehr gestreckt sind, und in einzelnen Abschnitten die Spiralfasern auftreten. Namentlich mache ich Sie aufmerksam auf die kleinen Auswüchse, welche überall am Rande hervortreten, ganz ähnlich gewissen thierischcn Excrescenzen, z.B. an den Zotten des Chorions, wo sie die Orte bezeichnen, an welchen die jungen Aeste hervortreten werden. An einzelnen Stellen unseres Ligustrum-Objectes finden sich nämlich kleine, kolbige Zapfen, die sich in gewissen Abständen wiederholen, nach Innen mit den |
[19] Zellenreihen des Parenchyms zusammenhängend. Dies sind
Bildungen, an denen man am besten die feineren Formen der
Zelle unterscheiden und zugleich die eigenthümliche Art des
Wachsthums entdecken kann. Das Wachsthum geht so vor
sich, dass an einzelnen zelligen Elementen eine Theilung eintritt
und sich eine quere Scheidewand bildet; die Theile wachsen
als selbständige Elemente fort und vergrössern sich nach und
nach. Nicht selten treten auch Längstheilungen ein, so dass
die Theile dicker werden. Jeder Zapfen ist also ursprünglich
eine Zelle, die, indem sie sich quertheilt und immer wieder
quertheilt, ihre Glieder vorwärts schiebt und dann bei Gelegenheit
auch seitlich sich ausbreitet. In dieser Weise wachsen
die Zapfen hervor, und dies ist im Allgemeinen der Modus
des Wachsthums nicht nur in der Pflanze, sondern auch
in den physiologischen und pathologischen Bildungen des thierischen
Leibes.
Beim folgenden Präparate, einem Stück Rippenknorpel im
Stadium des pathologischen Wachsthums, erscheinen schon
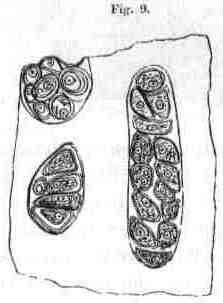 |
Veränderungen für das blosse Auge: kleine Buckel auf der Fläche des Knorpels. Dem ent- sprechend zeigt das Mikroskop Wucherungen der Knorpelzellen. Hier finden sich dieselben Formen wie bei den Pflanzenzellen, grössere Gruppen von zelligen Elementen, welche in mehrfachen Reihen angeordnet sind; mit dem einzigen Unterschiede von den wuchernden Pflanzenzellen, dass |
[20] zwischen den einzelnen Gruppen Intercellularsubstanz vorhanden
ist. An den Zellen unterscheidet man wieder die äussere
Kapsel, die sogar an einzelnen Zellen mehrfach geschichtet
ist, in 2-, 3- und mehrfacher Lage, und darin erst kommt die
eigentliche Zelle mit Membran, Inhalt, Kern und Kernkörperchen.
In dem folgenden Objecte sehen Sie junge Eierstockseier
des Frosches, bevor die Abscheidung der Dotterkörner begonnen
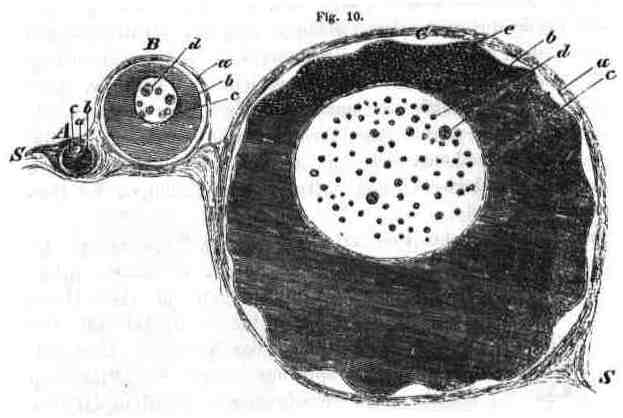
hat. Die sehr grosse Eizelle enthält einen gleichfalls sehr
grossen Kern, in dem eine Menge von kleinen Bläschen vertheilt
sind, und einen ziemlich dicken, trüben Inhalt, der an
einer bestimmten Stelle körnig und braun zu werden anfängt.
Um sie herum bemerkt man das verhältnissmässig schwache
Bindegewebe des Graaf’schen Follikels, mit einem schwer zu
erkennenden Epithelial-Stratum. Daneben liegen mehrere
kleinere Eier, welche dass allmählige Wachsthum erkennen
lassen.
[21] Im Gegensatze zu diesen colossalen Zellen lege ich Ihnen
noch ein klinisches Object vor: Zellen von einem frischen
katarrhalischen Sputum. Sie sehen im Verhältniss sehr kleine
Elemente, die sich bei stärkerer Vergrösserung als vollkommen
 |
runde Formen darstellen, und an denen man, nach Einwirkung von Wasser und Reagentien, deutlich eine Membran, Kerne und einen im frischen Zustande trüben Inhalt unterscheidet. Die meisten von den kleinen Elementen gehören nach der gewöhnlichen Terminologie in die Reihe der |
Eiterkörperchen; die grösseren, als Schleimkörperchen oder
katarrhalische Zellen zu bezeichnen, enthalten zum Theil Fett
oder grauschwarzes Pigment in Form von Körnern.
Diese Formen haben, so klein sie sind, doch die ganze
typische Eigenthümlichkeit der grossen; alle Zellencharaktere
der grossen finden sich an ihnen wieder. Das ist aber meines
Erachtens das Wesentliche, dass, wir mögen nun die grossen
oder die kleinen, die pathologischen oder physiologischen
Zellen zusammenhalten, wir dies Uebereinstimmende immer
wiederfinden.
[4Anm] Fig. 1. Pflanzenzellen aus dem Centrum des jungen Triebes eines
Knollens von Solanum tuberosum. a. die gewöhnliche Erscheinung des
regelmässig polygonalen, dickwandigen Zellengewebes, b. eine isolirte
Zelle mit feinkörnigem Aussehen der Höhlung, in der ein Kern mit
Kernkörperchen zu sehen ist. c. dieselbe Zelle, nach Einwirkung von
Wasser, der Inhalt (Protoplasma) hat sich von der Wand (Membran,
Capsel) zurückgezogen. An seinem Umfange ist eine besondere feine
Haut (Primordialschlauch) zum Vorschein gekommen. d. dieselbe Zelle
bei längerer Einwirkung von Wasser; die innere Zelle (Protoplasma mit
Primordialschlauch und Kern) hat sich ganz zusammengezogen und ist
nur durch feine, zum Theil ästige Fäden mit der Zellhaut (Capsel) in
Verbindung geblieben.
[6Anm] Fig. 2. Knorpelzellen, wie sie am Ossificationsrande wachsender
Knorpel vorkommen, ganz den Pflanzenzellen analog (vgl. die Erklärung
zu Fig. 1.). a–c. entwickeltere, d. jüngere Form.
[8Anm] Fig. 3. a. Leberzelle. b. Spindelzelle des Bindegewebes. c. Capillargefäss.
d. Grössere Sternzelle aus einer Lymphdrüse. e. Ganglienzelle
aus dem Kleinhirn. Die Kerne überall gleichartig.
[9Anm] Fig. 4. Nach Schleiden, Grundzüge der wiss. Botanik I. Fig. 1.
“Inhalt des Embryosackes von Vicia faba bald nach der Befruchtung. In
der hellen, aus Gummi und Zucker bestehenden Flüssigkeit schwimmen
Körnchen von Proteinverbindungen (a), unter denen sich einzelne grössere
auffallend auszeichnen. Um diese letzteren sieht man dann die ersteren
zu einer kleinen Scheibe zusammengeballt (b. c.). Um andere Scheiben
erkennt man einen hellen, scharf begrenzten Saum, der sich allmählich
weiter von der Scheibe (dem Cytoblasten) entfernt und endlich
deutlich als junge Zelle (d. e.) erkannt wird.”
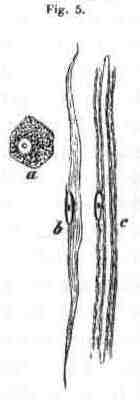
[11Anm] Fig. 5. a. Pigmentzelle aus der Choroides oculi. b. Glatte Muskelzelle
aus dem Darm. c. Stück einer doppeltcontouirten Nervenfaser
mit Axencylinder, Markscheide und wandständigem, nucleolirtem Kern.
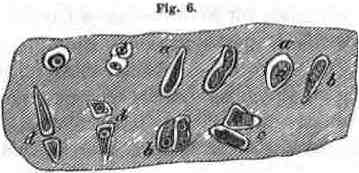
[13Anm] Fig. 6. Epiphysenknorpel vom Oberarme eines Kindes, an der Ellenbeuge.
Das Object war zuerst mit chromsaurem Kali und dann mit Essigsäure
behandelt. In der homogenen Grundsubstanz (Intercellulargewebe)
sieht man bei a. Knorpelhöhlen mit noch dünner Wand (Capsel),
in welchen die Knorpelzellen, mit Kern und Kernkörperchen versehen,
sich deutlich abgrenzen. b. Capseln (Höhlen) mit zwei, durch Theilung
der früher einfachen, entstandenen Zellen. c. Theilung der Capseln
nach Theilung der Zellen. d. Auseinanderrücken der getheilten
Capseln durch Zwischenlagerung von Intercellularsubstanz. —
Knorpelwachsthum.
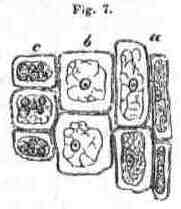
[17Anm] Fig. 7. Aus der Rindenschicht eines Knollens von Solanum tuberosum
nach Behandlung mit Jod und Schwefelsäure. a Platte Rindenzellen,
umgeben von der Kapsel (Zellhaut, Membran). b. Grössere, viereckige
Zellen derselben Art; die goschrumpfte und gerunzelte eigentliche
Zelle (Primordialschlauch) innerhalb der Kapsel. c. Zelle mit
Amylonkörnern, welche innerhalb des Primordialschlauches liegen.
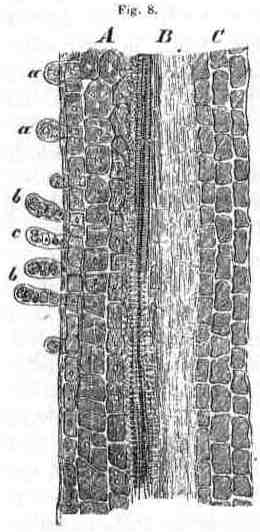
[18Anm] Fig. 8. Längsschnitt durch einen jungen Februar-Trieb vom Aste
eines Ligustrum. A. die äussere Schicht: unter einer sehr platten Zellenlage
sieht man grössere, viereckige, kernhaltige Zellen, aus denen
durch fortgehende Quertheilung kleine Zapfen (a) hervorwachsen, die
[19Anm] immer länger werden (b) und durch Längstheilung sich verdicken (c).
B. die Gefässschicht mit Spiralfasern. C. einfache, viereckige, längliche
Zellen. — Pflanzenwachsthum.
Fig. 9. Knorpelwucherung aus dem Rippenknorpel eines Erwachsenen.
Grössere Gruppen von Knorpelzellen innerhalb einer gemeinschaftlichen
Umgrenzung (falschlich (!) sogenannte Mutterzelle), durch successive
Theilungen aus einzelnen Zellen hervorgegangen. Am Rande davon ist
eine solche Gruppe durchschnitten, in der man eine Knorpelzelle mit
mehrfacher Umlagerung von Kapselschichten (äusserer Absonderungsmasse)
sieht. Vergröss. 300.
[20Anm] Fig. 10. Junge Eierstockseier vom Frosch. A. eine ganz junge
Eizelle. B. eine grössere. C. eine noch grössere mit beginnender Abscheidung
brauner Körnchen an dem einen Pol (e) und mit äusserer Einfaltung
der Zellmembran durch Eindringen von Wasser. a. Membran
des Follikels. b. Zellmembran. c. Kernmembran. d. Kernkörperchen.
S. Eierstock. Vergröss. 150.
[21Anm] Fig. 11. Zellen aus frischem katarrhalischen Sputum. A. Eiterkörperchen.
a. ganz frisch. b. nach Behandlung mit Essigsäure: in der
Membran ist der Inhalt aufgeklärt und man sieht drei kleine Kerne.
B. Schleimkörperchen. a. einfaches. b. mit Pigmentkörnchen. Vergr. 300.
13 Most Intelligent People In The History Of The World
https://financesonline.com/13-most-intelligent-people-in-the-history-of-the-world/